
19 results
Clostridioides difficile infection surveillance in intensive care units and oncology wards using machine learning
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 11 / November 2023
- Published online by Cambridge University Press:
- 24 April 2023, pp. 1776-1781
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prospective evaluation of data-driven models to predict daily risk of Clostridioides difficile infection at 2 large academic health centers – ERRATUM
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 10 / October 2023
- Published online by Cambridge University Press:
- 19 December 2022, p. 1705
- Print publication:
- October 2023
-
- Article
-
- You have access
- HTML
- Export citation
Prospective evaluation of data-driven models to predict daily risk of Clostridioides difficile infection at 2 large academic health centers
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 7 / July 2023
- Published online by Cambridge University Press:
- 19 September 2022, pp. 1163-1166
- Print publication:
- July 2023
-
- Article
- Export citation
The prescriber’s guide to classic MAO inhibitors (phenelzine, tranylcypromine, isocarboxazid) for treatment-resistant depression
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 4 / August 2023
- Published online by Cambridge University Press:
- 15 July 2022, pp. 427-440
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Self-blame in major depression: a randomised pilot trial comparing fMRI neurofeedback with self-guided psychological strategies
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 7 / May 2023
- Published online by Cambridge University Press:
- 02 December 2021, pp. 2831-2841
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Admission and Discharge Sampling Underestimates Multidrug-Resistant Organism (MDRO) Acquisition in an Intensive Care Unit
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
-
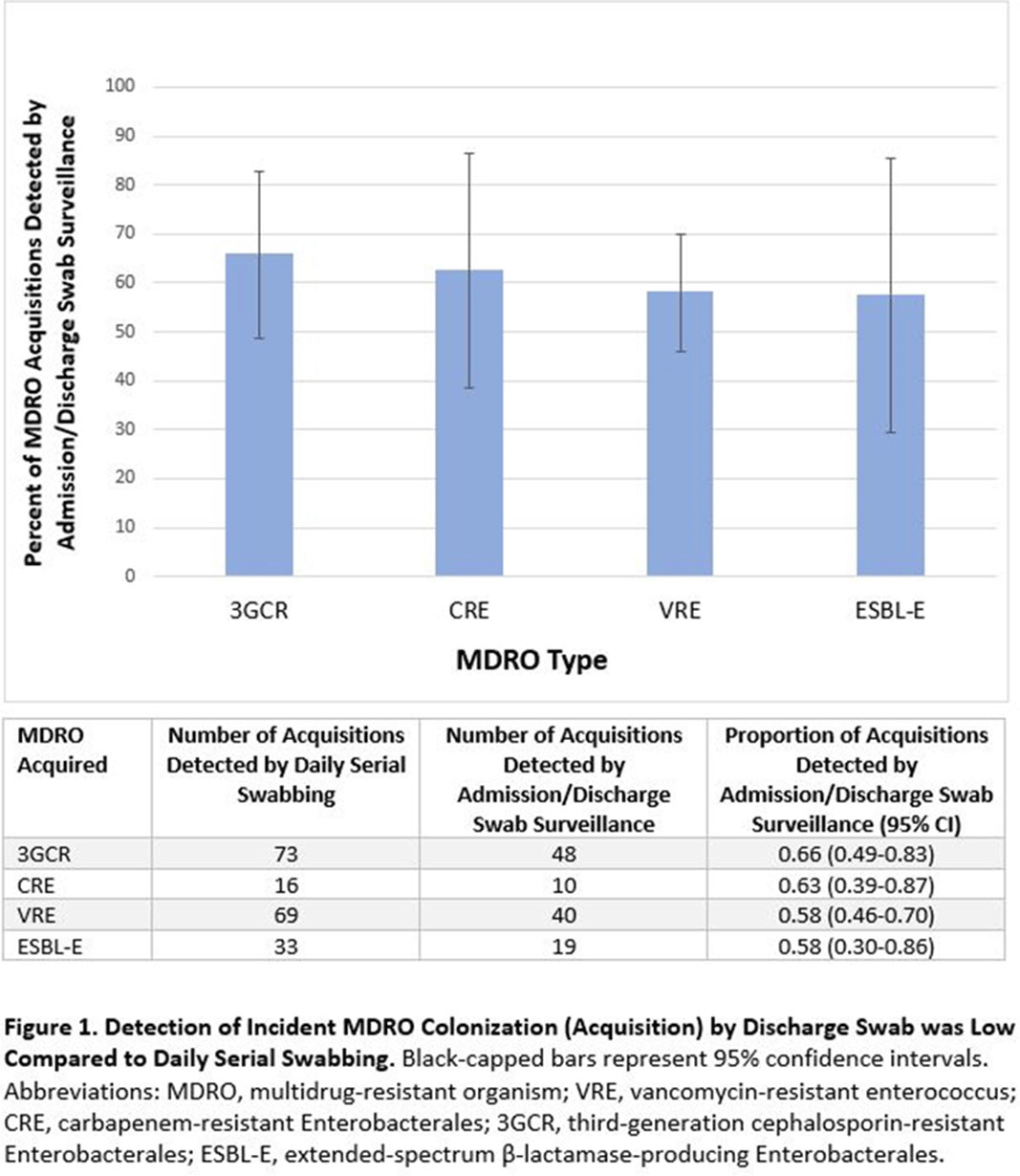
Background: Identification of hospitalized patients with enteric multidrug-resistant organism (MDRO) carriage, combined with implementation of targeted infection control interventions, may help reduce MDRO transmission. However, the optimal surveillance approach has not been defined. We sought to determine whether daily serial rectal surveillance for MDROs detects more incident cases (acquisition) of MDRO colonization in medical intensive care unit (MICU) patients than admission and discharge surveillance alone. Methods: Prospective longitudinal observational single-center study from January 11, 2017, to January 11, 2018. Inclusion criteria were ≥3 consecutive MICU days and ≥2 rectal or stool swabs per MICU admission. Daily rectal or stool swabs were collected from patients and cultured for MDROs, including vancomycin-resistant Enterococcus (VRE), carbapenem-resistant Enterobacterales (CRE), third-generation cephalosporin-resistant Enterobacterales (3GCR), and extended-spectrum β-lactamase–producing Enterobacterales (ESBL-E) (as a subset of 3GCR). MDRO detection at any time during the MICU stay was used to calculate prevalent colonization. Incident colonization (acquisition) was defined as new detection of an MDRO after at least 1 prior negative swab. We then determined the proportion of prevalent and incident cases detected by daily testing that were also detected when only first swabs (admission) and last swabs (discharge) were tested. Data were analyzed using SAS version 9.4 software. Results: In total, 939 MICU stays of 842 patients were analyzed. Patient characteristics were median age 64 years (interquartile range [IQR], 51–74), median MICU length of stay 5 days (IQR, 3–8), median number of samples per admission 3 (IQR, 2–5), and median Charlson index 4 (IQR, 2–7). Prevalent colonization with any MDRO was detected by daily swabbing in 401 stays (42.7%). Compared to daily serial swabbing, an admission- and discharge-only approach detected ≥86% of MDRO cases (ie, overall prevalent MDRO colonization). Detection of incident MDRO colonization by an admission- or discharge-only approach would have detected fewer cases than daily swabbing (Figure 1); ≥34% of total MDRO acquisitions would have been missed. Conclusions: Testing patients upon admission and discharge to an MICU may fail to detect MDRO acquisition in more than one-third of patients, thereby reducing the effectiveness of MDRO control programs that are targeted against known MDRO carriers. The poor performance of a single discharge swab may be due to intermittent or low-level MDRO shedding, inadequate sampling, or transient MDRO colonization. Additional research is needed to determine the optimal surveillance approach of enteric MDRO carriage.
Funding: No
Disclosures: None
Figure 1.

95332 Intestinal inflammation and altered gut microbiota associated with inflammatory bowel disease render mice susceptible to Clostridioides difficile colonization and infection
-
- Journal:
- Journal of Clinical and Translational Science / Volume 5 / Issue s1 / March 2021
- Published online by Cambridge University Press:
- 31 March 2021, p. 90
-
- Article
-
- You have access
- Open access
- Export citation
54101 Characterizing Microbiota Features of Clostridioides difficile Infections
-
- Journal:
- Journal of Clinical and Translational Science / Volume 5 / Issue s1 / March 2021
- Published online by Cambridge University Press:
- 31 March 2021, p. 89
-
- Article
-
- You have access
- Open access
- Export citation
Genomic Epidemiology of Clostridioides difficile Sequence Types 1 and 2 Across Three US Medical Centers
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s238
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Recurrent Clostridioides difficile infection can be predicted using inflammatory mediator and toxin activity levels
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s77-s78
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Blind Spots in Methods Based on Cultivation and Metagenomic Sequencing for Surface Microbiomes in a Medical Intensive Care Unit
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s141-s142
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
3343 Identification of host-microbial interaction networks that mediate intestinal epithelial barrier function in necrotizing enterocolitis
-
- Journal:
- Journal of Clinical and Translational Science / Volume 3 / Issue s1 / March 2019
- Published online by Cambridge University Press:
- 26 March 2019, p. 13
-
- Article
-
- You have access
- Open access
- Export citation
3185 A Randomized Controlled Trial Comparing the Nonabsorbable Antibiotic Rifaximin vs. Dietary Intervention Low in Fermentable Sugars (FODMAP) in Irritable Bowel Syndrome
-
- Journal:
- Journal of Clinical and Translational Science / Volume 3 / Issue s1 / March 2019
- Published online by Cambridge University Press:
- 26 March 2019, p. 31
-
- Article
-
- You have access
- Open access
- Export citation
A Generalizable, Data-Driven Approach to Predict Daily Risk of Clostridium difficile Infection at Two Large Academic Health Centers
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 39 / Issue 4 / April 2018
- Published online by Cambridge University Press:
- 26 March 2018, pp. 425-433
- Print publication:
- April 2018
-
- Article
-
- You have access
- HTML
- Export citation
Fecal Microbiota Therapy: Ready for Prime Time?
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 35 / Issue 1 / January 2014
- Published online by Cambridge University Press:
- 10 May 2016, pp. 28-30
- Print publication:
- January 2014
-
- Article
- Export citation
Detection of Mixed Populations of Clostridium difficile from Symptomatic Patients Using Capillary-Based Polymerase Chain Reaction Ribotyping
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 34 / Issue 9 / September 2013
- Published online by Cambridge University Press:
- 02 January 2015, pp. 961-966
- Print publication:
- September 2013
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Christianity
- Published online:
- 05 August 2012
- Print publication:
- 20 September 2010, pp xi-xliv
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- The Cambridge Handbook of Forensic Psychology
- Published online:
- 06 July 2010
- Print publication:
- 29 April 2010, pp xix-xxiii
-
- Chapter
- Export citation
Explaining unexplained diarrhea and associating risks and infections
-
- Journal:
- Animal Health Research Reviews / Volume 8 / Issue 1 / June 2007
- Published online by Cambridge University Press:
- 13 August 2007, pp. 69-80
-
- Article
- Export citation
